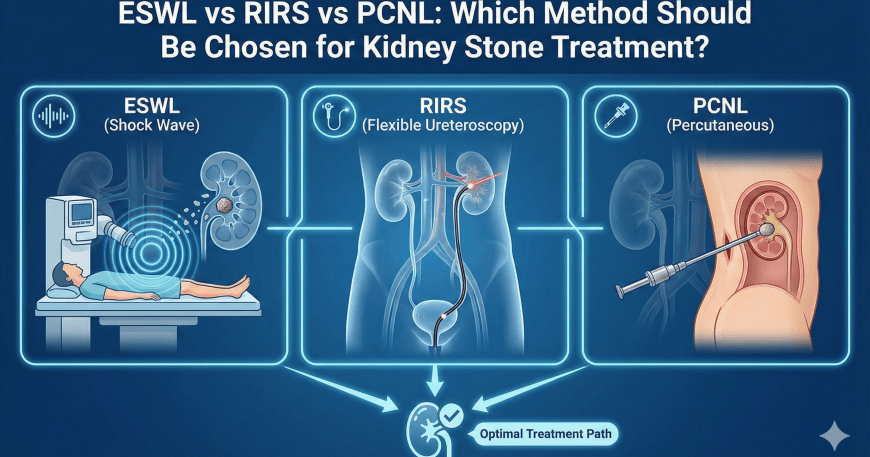
ESWL (Shock Wave Lithotripsy) vs RIRS vs PCNL: Which Method Should Be Chosen for Kidney Stone Treatment?
In the management of renal and ureteral stone disease, there is no single “best” treatment for every patient. The optimal modality is determined by a comprehensive assessment of stone size, location, composition/hardness, the presence of obstruction and/or infection, as well as patient-specific factors. In my clinical practice, the primary goal is to achieve the highest possible stone-free rate with the safest approach, while enabling the patient to return to daily life as quickly as possible.
In this article, I outline the three most commonly used modalities—ESWL (Extracorporeal Shock Wave Lithotripsy), RIRS (Retrograde Intrarenal Surgery using flexible ureteroscopy and laser lithotripsy), and PCNL (Percutaneous Nephrolithotomy)—and explain the rationale for selecting each method in different clinical scenarios.
Key determinants of treatment selection
1) Stone size
- Small stones (often <10 mm): in selected patients, observation/medical expulsive strategies may be appropriate; if intervention is required, ESWL or RIRS can be considered depending on stone and patient characteristics.
- Intermediate-sized stones (approximately 10–20 mm): endoscopic approaches frequently provide higher efficacy and better predictability.
- Large stones (particularly ≥2 cm or staghorn calculi): PCNL is commonly favored to maximize stone clearance in a timely manner.
2) Stone location
Stone location within the kidney (upper/mid/lower calyx, renal pelvis) or within the ureter (proximal, mid, distal) directly influences the choice of treatment. For example, lower pole stones may be more challenging to clear with certain modalities due to unfavorable anatomy and fragment clearance dynamics.
3) Stone hardness / composition
Stone density (e.g., on non-contrast CT) and suspected composition are important predictors of response, particularly for ESWL, where success is closely linked to stone fragility.
4) Obstruction and infection
If stone disease is accompanied by fever, rigors, signs of urinary tract infection, and/or significant hydronephrosis, the priority is not immediate stone fragmentation, but urgent decompression of the collecting system and infection control. In appropriate cases, urinary drainage may be established with a ureteral stent or percutaneous nephrostomy prior to definitive stone treatment.
5) Patient-related factors
Anticoagulant use, pregnancy, solitary kidney, baseline renal function, obesity, and prior urologic interventions can materially alter the risk–benefit balance and therefore the treatment plan.
What is ESWL? (Extracorporeal Shock Wave Lithotripsy)
ESWL is a non-invasive technique that uses externally generated shock waves to fragment urinary stones, allowing the resulting fragments to pass spontaneously through the urinary tract. No incision is required, and it can be an effective option in appropriately selected patients.
When I most commonly consider ESWL
- The stone is small to intermediate in size
- The stone is expected to be sufficiently fragmentable (favorable density/composition)
- Stone location and renal anatomy are conducive to fragment clearance
- There is no active infection and no high-risk obstruction requiring urgent drainage
Practical considerations with ESWL
- Multiple sessions may be required.
- Fragment passage can trigger renal colic.
- Complete clearance is not guaranteed; if residual stone burden persists, endoscopic management is often the next step.
What is RIRS? (Retrograde Intrarenal Surgery)
RIRS involves retrograde access to the upper urinary tract via the urethra and ureter using a flexible ureteroscope. Stones are visualized directly and treated with laser lithotripsy, with fragment extraction when feasible. A temporary double-J ureteral stent may be placed depending on intraoperative findings and anticipated postoperative ureteral edema.
When I most commonly consider RIRS
- Renal stones where a controlled endoscopic approach is desirable
- Scenarios where ESWL is expected to have a low probability of success
- Intermediate-sized renal stones (often in the ~1–2 cm range), depending on anatomy and stone burden
- Cases requiring direct visualization and more predictable clearance compared with ESWL
Postoperative course after RIRS
- Many patients resume routine activities relatively quickly.
- If a stent is placed, transient symptoms such as urinary frequency, dysuria, and flank/groin discomfort may occur.
- With higher stone burden, a staged procedure (second session) may be necessary.
What is PCNL? (Percutaneous Nephrolithotomy)
PCNL is a minimally invasive surgical approach that provides direct access to the renal collecting system through a small flank tract. Stones are fragmented and removed, making PCNL particularly effective for patients with large or complex stone burden. It is generally the modality that offers the highest likelihood of achieving a stone-free state in a single treatment course for large stones.
When I most commonly consider PCNL
- Stones ≥2 cm
- Multiple renal stones with substantial overall stone burden
- Staghorn (branched) calculi
- Significant residual stone burden after other modalities
Practical considerations with PCNL
- It is more invasive than ESWL and RIRS.
- The risk of bleeding is higher relative to the other options, and careful preoperative evaluation is essential.
- Hospital stay is often somewhat longer.
- In selected cases, a temporary nephrostomy tube may be used postoperatively.
How do I decide among these options? A clinical framework
In general terms:
- Small, favorable stones: ESWL or RIRS
- Intermediate renal stones: RIRS often provides a controlled and effective option
- Large stones / multiple stones / staghorn stones: PCNL is frequently the most appropriate approach
The overarching principle is not to choose the “easiest” procedure, but to select the modality that offers the best balance of safety, efficacy, and durable stone clearance for the individual patient.
When is urgent evaluation required?
Prompt medical assessment is warranted if any of the following occur:
- Fever or rigors
- Severe pain with persistent nausea/vomiting or inability to maintain hydration
- Marked reduction in urine output or inability to void
- Symptoms in a patient with a solitary kidney
- Suspected stone disease during pregnancy
Conclusion
ESWL, RIRS, and PCNL are all highly effective modalities when applied to the appropriate patient and stone profile. My approach is to tailor treatment based on imaging—particularly non-contrast CT—clinical status, and individual risk factors, aiming for the highest stone-free outcome using the safest feasible strategy.