Peyronie’s Disease: Does Penile Curvature Resolve Spontaneously?
Peyronie’s disease (PD) is one of the most underreported urological conditions in clinical practice, as many patients hesitate to discuss it due to embarrassment. Nonetheless, recent epidemiological studies demonstrate a prevalence of 3% to 9% in the adult male population—meaning at least one in every twenty men will face this condition at some point in their lifetime.
The question patients most frequently raise during initial consultation is almost invariably the same: “Doctor, will this curvature resolve on its own?” Drawing on over 25 years of clinical experience and the current evidence-based literature, this article offers a comprehensive answer to that question.
What Is Peyronie’s Disease?
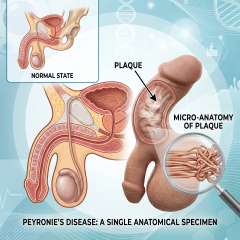
Peyronie’s disease is characterized by the formation of a fibrous plaque within the tunica albuginea, the fibroelastic sheath enveloping the corpora cavernosa of the penis. This plaque compromises the elasticity of the tunica and leads to penile curvature, shortening, or deformity during erection.
Although the condition was first described by the French surgeon François Gigot de la Peyronie in 1743, its underlying pathophysiology has only been elucidated over the past three decades. Current evidence confirms that PD is not merely a mechanical curvature disorder but rather a genuine connective tissue disease with systemic implications.
Clinical Manifestations of Peyronie’s Disease
The clinical presentation of PD varies considerably among patients. The most frequently encountered symptoms include:
- Penile curvature during erection (dorsal, ventral, lateral, or multidirectional)
- Palpable fibrous plaque beneath the penile skin
- Pain during erection (penile pain)
- Reduction in penile length
- Circumferential narrowing or “hourglass” deformity
- Diminished erectile rigidity (observed in approximately 40% of cases)
- Difficulty or discomfort during sexual intercourse
Etiology of Peyronie’s Disease
The etiology of PD is multifactorial, arising from the interplay of several predisposing factors. The principal risk factors include:
Microtrauma: Repetitive microtrauma to the tunica albuginea during sexual intercourse—particularly from buckling injury—is recognized as the most prevalent triggering mechanism. In genetically predisposed individuals, aberrant wound healing following these microtears results in plaque formation.
Genetic predisposition: Men with Dupuytren’s contracture exhibit an approximately fourfold increased risk of developing PD. This association supports the hypothesis that PD represents a genetically mediated connective tissue disorder.
Age: The incidence rises significantly between the ages of 50 and 70, though the condition may also manifest in men in their third decade of life.
Comorbid conditions: Diabetes mellitus, hypertension, hypogonadism, and tobacco use are significant contributors to both disease onset and progression.
Post-surgical etiology: The literature reports a 15–16% incidence of PD following radical prostatectomy.
Acute vs. Chronic Phase: The Critical Distinction That Guides Treatment
The most essential concept to understand regarding Peyronie’s disease is that it encompasses two distinctly different phases, each dictating a fundamentally different therapeutic approach. A significant proportion of inappropriate treatment decisions stem from inadequate recognition of this dichotomy.
Acute (Active) Phase: The First 12–18 Months
This phase extends approximately 12 to 18 months from symptom onset, during which the plaque remains biologically “active.” Its characteristic features include:
- Presence of penile pain during erection or at rest
- Progressive variation in curvature angle (either worsening or occasionally improving)
- Soft plaque consistency with indistinct borders
- Ongoing inflammatory activity within the tunica
Surgical intervention is strictly contraindicated during this phase, as the disease has not yet stabilized, and the risk of postoperative recurrence is substantially elevated.
Chronic (Stable) Phase: Beyond 12–18 Months
In this phase, the plaque has matured and transformed into dense scar tissue:
- Pain has generally resolved completely
- Curvature has remained unchanged for at least 3–6 months
- The plaque is firm, with well-defined borders on palpation
- Inflammatory activity has subsided, diminishing the efficacy of conservative therapies
The therapeutic paradigm in the chronic phase shifts entirely; the objective is no longer to control inflammation but to correct the established deformity.
Does Peyronie’s Disease Resolve Spontaneously?
We now turn to the central question. Contrary to the misconceptions frequently encountered in clinical practice, the current literature is unambiguous on this point.
Epidemiological Evidence
Data endorsed by the European Association of Urology (EAU) and the American Urological Association (AUA) guidelines demonstrate the following natural history in untreated patients:
- 12–13% experience spontaneous improvement in curvature
- 40–50% remain stable over time
- 30–50% demonstrate progressive worsening of the deformity
In other words, only one in ten patients exhibits meaningful spontaneous resolution. This rate is insufficient to justify a “watch-and-wait” strategy as a standard approach.
Patient Profile Favoring Spontaneous Resolution
Based on clinical experience, the patient profile most likely to achieve spontaneous improvement includes:
- Younger age (below 40 years)
- Early disease (within the first 6 months)
- Curvature less than 20 degrees
- Small plaque size (less than 1 cm)
- Absence of calcification
- No concomitant metabolic comorbidities such as diabetes
Even in patients fitting this profile, early intervention has been shown to significantly enhance therapeutic outcomes.
Treatment of Peyronie’s Disease: Phase-Specific Protocols
Treatment Options in the Acute Phase
The principal objectives in this phase are suppression of inflammation, arrest of plaque progression, and pain management.
Oral pharmacotherapy: Pentoxifylline, low-dose daily tadalafil, and coenzyme Q10 are utilized for their anti-inflammatory and antifibrotic properties. Although their effects are modest, early administration may slow disease progression.
Intralesional injections: Intraplaque injections of verapamil or interferon alpha-2b offer moderate efficacy. Clinical trials have reported curvature improvement of 20–30%.
Clostridium histolyticum collagenase (CCH/Xiaflex): This remains the only FDA-approved pharmacological agent for PD. It is indicated for patients with curvature of 30 degrees or greater, a palpable plaque, and disease in the chronic phase. A four-cycle treatment protocol yields a mean curvature improvement of approximately 17 degrees.
Mechanical traction and vacuum devices: When applied for 3–8 hours daily, traction therapy may achieve curvature reduction of 10–20 degrees and length gain of 1–2 cm in early disease. However, treatment success is highly dependent on patient adherence.
Extracorporeal shock wave therapy (ESWT): While effective for pain management, its impact on curvature correction remains limited.
Treatment Options in the Chronic Phase
Once the plaque has stabilized, the response rate to conservative therapies decreases substantially. Surgical options therefore become the mainstay of treatment.
Plication procedures (Nesbit, Yachia): These techniques are preferred in patients with curvature below 60 degrees and adequate penile length. Sutures are placed on the contralateral tunica to straighten the penis. Reported success rates range from 85% to 95%.
Plaque incision/excision with grafting: This approach is indicated in patients with curvature greater than 60 degrees, hourglass deformity, or significant shortening. The plaque is incised or excised and replaced with either a biological or synthetic graft.
Penile prosthesis implantation: This represents the gold standard in patients with PD accompanied by significant erectile dysfunction. Concomitant manual modeling during implantation allows simultaneous correction of the curvature.
When Should You Consult a Urologist?
I recommend prompt consultation with a urologist upon noticing any of the following symptoms:
- New-onset penile pain during erection
- Palpable induration beneath the penile skin
- Visible curvature during erection
- Perceived reduction in penile length
- Difficulty during intercourse or partner complaints
Early diagnosis directly influences treatment success. Clinical studies have demonstrated that treatment initiated within the first six months is two to three times more effective than treatment initiated in advanced disease.
Frequently Asked Questions
Is Peyronie’s disease a form of cancer?
No. PD is an entirely benign connective tissue disorder with no risk of malignant transformation. Nevertheless, any sudden plaque enlargement or change in pain pattern warrants prompt evaluation.
Does vitamin E improve Peyronie’s disease?
Vitamin E, previously recommended in older guidelines, has failed to demonstrate efficacy in placebo-controlled trials over the past two decades. The current EAU guidelines do not recommend vitamin E monotherapy.
Is Peyronie’s disease sexually transmitted?
No. PD is not a communicable disease; it develops secondary to microtrauma and genetic predisposition.
Can masturbation cause Peyronie’s disease?
Normal masturbatory practices do not cause PD. However, the application of excessive force or sudden bending of the erect penis may induce microtrauma and thereby predispose to the condition.
Does surgical correction of Peyronie’s disease impair sexual function?
In experienced hands, the risk of postoperative erectile dysfunction following plication procedures is less than 5%. For grafting procedures, this rate may rise to approximately 20%, underscoring the importance of appropriate patient selection.
Is Peyronie’s disease treatment covered by insurance?
Surgical interventions and certain oral medications are generally covered by most health insurance plans. However, collagenase injections and traction devices are frequently out-of-pocket expenses.
Conclusion
Peyronie’s disease demonstrates spontaneous resolution in only 1 out of 10 patients, yet it can be substantially controlled with early and appropriately targeted therapy. Rather than adopting a “wait-and-see” approach, clinicians must determine whether the patient is in the acute or chronic phase and develop a personalized treatment plan accordingly.
It is important to remember that Peyronie’s disease is not a condition to be concealed in silence. Thousands of men successfully manage this condition each year. Early consultation not only reduces the need for surgical intervention but also significantly preserves sexual function and quality of life.